| 알파스팀(Alpha-Stim)에 대해서 | 목록으로 가기 |
두개 전기 요법 자극으로 섬유근육통 치료
date: 2022.05.02
Lichtbroun, Alan S., Raicer, Mei-Ming C. 및 Smith, Ray B. 뇌 전기 요법 자극으로 섬유 근육통 치료. 임상 류마티스 저널. 2001년; 7(2):72-78. 1999년 10월 뉴욕 컬럼비아 대학교에서 열린 침술 및 전기 요법에 관한 제15회 연례 국제 심포지엄에서 발표되었습니다.
장치
알파 스팀(Alpha-Stim)®
주요 변수
불안, 수면의 질(불면증) 및 우울증
목적
섬유근육통 환자의 수면의 질, 불안, 우울, 분노, 압통점 점수, 자가 평가된 통증, 활력, 피로, 혼란, 웰빙 느낌 및 삶의 질에 대한 CES의 특정 치료 과정의 효과를 평가하기 위해 포함 및 제외 기준을 충족하는 대상에서 동일한 실험 조건에서 가짜 치료와 비교했습니다.
테스트 설계
IRB는 3주간의 무작위 배정, 가짜 치료 대조, 이중 맹검 임상 시험을 포함하는 6주간의 연구에 이어 가짜 및 대조군의 피험자가 CES.
1차 유효성 결과
RCT의 1차 유효성 평가변수는 전반적인 통증, 수면의 질, 웰빙 및 삶의 질에 대한 10점 수치 평가 척도(NRS)에 대한 마지막 치료 후 자체 평가 점수의 기준선으로부터의 변화였습니다. 연구 3주차 말에 모의 치료군과 비교한 기분 상태(POMS) 하위척도의 프로필.
오픈 라벨 크로스오버 부문의 1차 유효성 평가변수는 10점 NRS(Numerical Rating Scale)에 대한 마지막 치료 후 점수의 기준선에서 전반적인 통증, 수면의 질 및 웰빙의 질에 대한 사후 테스트로의 변화였습니다. 연구 6주가 끝날 때 POMS 하위척도를 측정합니다. 효과 결과 측정은 RCT 연구의 3주가 끝날 때와 3주 후에 공개 라벨 교차 부문이 끝날 때 완료되었습니다.
주요 포함 기준
• 섬유근육통이 있는 21세 이상의 남성 및 여성 피험자.
• 섬유근육통 진단은 American College of Rheumatology에서 설정한 기준을 사용하여 보드 인증 류마티스 전문의에 의해 확인되었습니다.
• 섬유근육통 진단은 American College of Rheumatology에서 설정한 기준을 사용하여 보드 인증 류마티스 전문의에 의해 확인되었습니다.
주요 제외 기준
• 임신.
• 이식된 심박조율기, 펌프 또는 자극기의 존재.
• 이식된 심박조율기, 펌프 또는 자극기의 존재.
프로토콜 요약 무작위 배정은 연구 시작 전에 설정되었습니다. 1차 유효성 평가변수의 측정은 치료 기간 시작 전 기준선에서 수행되었습니다. 연구 동안 환자의 의학적 관리에 변화가 없었습니다. 프로토콜은 두 개의 암으로 구성되었습니다.
• RCT 암: 활성 CES 장치 또는 가짜 장치로 3주 치료. 베이스라인 테스트 후, 피험자들은 CES 장치를 사용하도록 교육받았고, 3주 동안 매일 1시간 동안 사용하도록 지시받았습니다. 3주가 끝나면 피험자는 진료소로 돌아와 결과 측정을 반복했습니다.
• 오픈 라벨 크로스오버 암: 이 시점에서 눈가림이 해제되었고 가짜 및 대조군의 피험자에게 3주 동안 활성 CES를 받을 수 있는 옵션이 주어졌습니다. 가짜 그룹의 40명 중 23명이 오픈 레이블 크로스오버 부문에 참여하도록 선택되었습니다. 피험자들은 3주 동안 매일 1시간 동안 CES 장치를 사용했습니다. 3주간의 공개 라벨 크로스오버 부문이 완료되었을 때, 피험자들은 연구 결과 측정에 대해 재검사를 받았습니다.
• 오픈 라벨 크로스오버 암: 이 시점에서 눈가림이 해제되었고 가짜 및 대조군의 피험자에게 3주 동안 활성 CES를 받을 수 있는 옵션이 주어졌습니다. 가짜 그룹의 40명 중 23명이 오픈 레이블 크로스오버 부문에 참여하도록 선택되었습니다. 피험자들은 3주 동안 매일 1시간 동안 CES 장치를 사용했습니다. 3주간의 공개 라벨 크로스오버 부문이 완료되었을 때, 피험자들은 연구 결과 측정에 대해 재검사를 받았습니다.
장치 응용 프로토콜
피험자들은 무작위로 3개의 개별 그룹, 하위 수준의 에테르 활성 CES, 컨테이너에서 피험자 이름을 뽑아서 가짜 그룹 또는 통제로 할당되었습니다. 활성 CES 장치는 무감각 수준인 100μA로 설정되었습니다. 가짜 장치는 활성 CES 장치와 모양이 동일했지만 전류를 전도하지 않는 이 연구를 위해 만든 이어 클립을 사용했습니다.
스터디 블라인드
피험자, 조사자, 의사 및 직원은 모두 장치의 신원에 대해 가렸습니다.
산출측정지표
기분 프로필(POMS) 하위 척도 A는 불안을 측정하는 데 사용되었고 POMS 하위 척도 D는 우울증을 측정하는 데 사용되었습니다. 수면의 질은 10점 수치 평가 척도로 측정되었습니다. 사용된 모든 척도는 신뢰성과 타당성을 확립했습니다(McNair et al., 2014, 1971; Farrar et al., 2008).
결과
피험자
총 60명의 피험자가 등록되었으며, 58명의 여성과 2명의 남성이 23-82세(남성 = 50)세 범위에서 등록되었습니다. 60명의 모든 피험자들은 3주차 방문이 끝날 때 마지막 치료가 완료되었을 때 사후 테스트를 완료했습니다. 평균 증상 지속 기간은 11년(1~40년 범위)이었습니다. 피험자들은 활성 CES 그룹(N=20), 가짜 그룹(N=20) 또는 대기줄 위약 대조군(N=20)으로 무작위 배정되었습니다.
기준 측정: 그룹 동등성
12가지 결과 측정에서 활성 CES와 가짜 치료 그룹 간에 기준선에서 통계적으로 유의한 차이가 없었습니다.
데이터 분석
2011년 12월에 Electromedical Products International, Inc.의 통계 컨설턴트인 Dr. Larry Price는 이 2001년 Lichtbroun 연구의 데이터를 재분석하여 이전에 보고된 결과를 확인하고 보다 포괄적인 설명을 제공할 수 있는 더욱 강력한 분석을 수행했습니다. 결과. 원시 데이터는 공분산 분석(ANCOVA) 및 Mann-Whitney U를 사용하여 분석되었습니다. 조사관은 원래 기준선 및 종료점 연구 결과를 비교하기 위해 일원 분산 분석(ANOVA)을 사용했습니다.
1차 효과 결과: 3주차
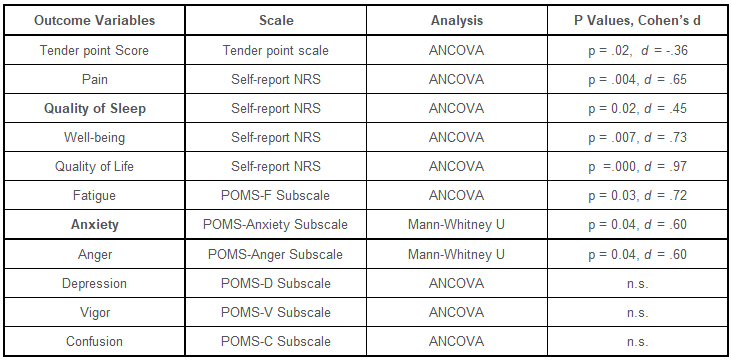
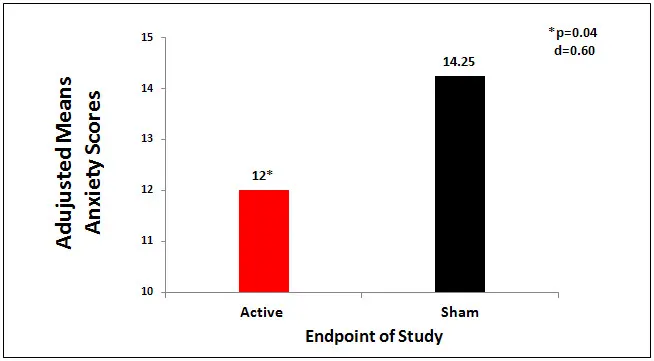
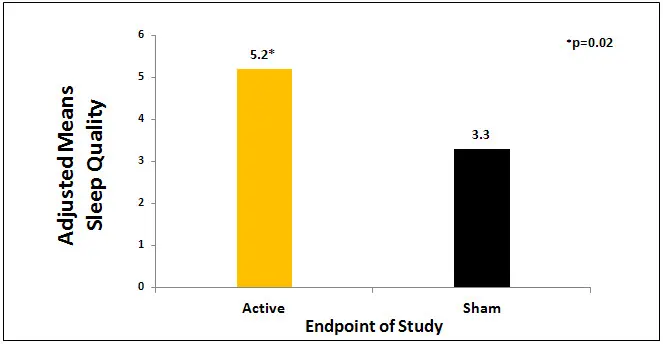
활동적인 CES 그룹은 sham 그룹과 비교하여 11개 변수 중 8개에서 유의미한 결과를 보였습니다: 유의하게 낮은 불안 점수(p=0.04, d = -.60), 높은 수면 품질 점수(p = 0.02, d = .45) , 낮은 통증 점수(p = .004, d = .65), 높은 웰빙 점수(p = .007, d = .73), 높은 삶의 질 점수(p = .000, d = .97) ), 가짜 그룹(표 1 참조)과 비교하여 낮은 피로 점수(p = 0.03, d = -.72 및 낮은 분노 점수(p = 0.04, d = .60). 활성 CES와 가짜 그룹 사이의 치료 효과 크기 범위 8개의 유의한 변수에 대해 -.36에서 .97, 통합 효과 크기는 .64입니다. 표 1은 결과 측정의 통계 분석 결과를 보여주고 그림 1과 그림 2는 불안 점수와 수면의 질에서 그룹 간의 결과를 보여줍니다.
 |
 |
 |
오픈 라벨 크로스오버 결과: 6주차
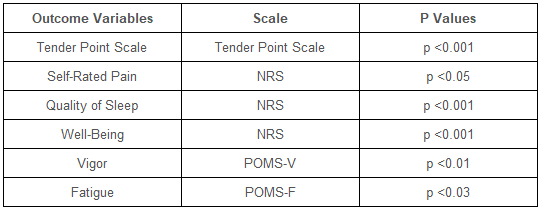
RCT 암 완료 후, 40명의 가짜 또는 대조군 환자 중 23명이 Alpha-Stim CES에 대한 표준 임상 프로토콜에 따라 전류를 증가시킬 수 있는 공개 라벨 교차 암에서 실제 CES를 선택했습니다. 데이터는 사후 테스트에서 최소 유의차와 함께 공분산 분산의 반복 측정 분석으로 분석되었습니다. 표 7은 6주차의 결과 측정에 대한 통계 분석 결과를 보여줍니다.
 |
연구의 가치
이 연구의 장점은 다음과 같습니다. 무작위, 가짜 대조, 이중 맹검 설계 사용(조사자는 연구에 Alpha-Stim RCT 연구 프로토콜을 사용하기로 선택했습니다); 활성 및 가짜 Alpha-Stim 장치는 공장에서 제조업체가 현재 수준 및 시간에 대해 각 특정 그룹에 대해 지정된 수준으로 미리 설정 및 잠그고 가짜 장치는 전기를 방출하지 않는 것을 제외하고 활성 장치와 동일합니다. 장치의 무작위화는 제조업체가 수행하고 조사자의 프로토콜에 따라 수행되었습니다. 3개의 그룹, 활성 가짜 및 대조군의 사용; 활성 그룹과 가짜 그룹 모두에 대한 CES 치료를 위한 구조화되고 상세한 프로토콜. 원본 데이터 분석의 한계는 분산 분석(ANOVA)을 사용하고 그룹 내 또는 그룹 효과 크기 사이가 포함되지 않았다는 것입니다. 2011년 데이터 재분석에서 ANCOVA(공분산 분석)를 사용하여 결과에 대한 보다 포괄적인 설명을 제공했습니다. 기분 상태 프로필(POMS) 하위 척도는 불안과 우울을 측정하는 데 사용되었습니다. 이것은 1990년대 후반과 2000년대 초반에 일반적인 접근 방식이었습니다. 오늘날에는 전적으로 불안에 초점을 맞춘 Hamilton Anxiety Rating Scale 또는 이와 유사한 등급 척도가 가장 많이 사용될 것입니다. 우울증의 변인을 측정할 때도 마찬가지이다. 우울증에 대한 CES의 효과는 우울증에 대한 다른 Alpha-Stim 연구의 결과와 대조적으로 이 연구에서 유의하지 않았습니다. 이 발견에 대한 한 가지 가능한 설명은 우울증에 대한 POMS 하위 척도의 사용인 반면, 다른 연구에서는 Hamilton Depression Rating Scale과 같이 우울증에 특별히 초점을 맞춘 척도를 사용했습니다. 이 연구에서 불안과 수면의 질에 대한 결과는 CES가 불안을 상당히 감소시키고 수면의 질을 향상시킨다는 다른 Alpha-Stim 연구의 결과와 일치합니다.
저자 소속
ASL, 로버트 우드 존슨 의과 대학, 이스트 브런즈윅, 뉴저지. MMC, Real Word Health, Wall, NJ. RBS, Electromedical Products International, Mineral Wells, TX,
참고문헌
Farrar JT, Troxel AB, Stott C, Duncombe P, Jensen MP. 경직의 0-10 숫자 등급 척도 측정에서 변경의 유효성, 신뢰성 및 임상적 중요성: 무작위, 이중 맹검, 위약 대조 시험의 사후 분석. 임상 치료학. 2008년 5월;30(5):974-85
McNair DM, Lorr M, Droppleman LF. Mood States 2nd Edition(POMS 2™) 프로필. JvR Psychometrics, 2014년 4월 18일에 액세스, http://www.psychologyafrica.com/wp-content/uploads/2013/07/Profile_of_Mood_States_2nd_Edition.pdf,
McNair DM, Lorr M, Droppleman LF. 기분 상태의 프로필 매뉴얼. 캘리포니아 샌디에고: 교육 및 산업 테스트 서비스, 1971.
원문보기
The treatment of fibromyalgia with cranial electrotherapy stimulation
Lichtbroun, Alan S., Raicer, Mei-Ming C., and Smith, Ray B. The treatment of fibromyalgia with cranial electrotherapy stimulation. Journal of Clinical Rheumatology. 2001; 7(2):72-78. Presented at the Fifteenth Annual International Symposium on Acupuncture and Electro-Therapeutics, Columbia University, New York, October 1999.
Device
Alpha-Stim®
Key Variables
Anxiety, Sleep Quality (Insomnia) and Depression
Objective
To evaluate the effect of a specified treatment course with CES on fibromyalgia patients’ sleep quality, anxiety, depression, anger, tender point scores, self-rated pain, vigor, fatigue, confusion, feelings of well-being, and quality of life when compared to sham treatment under the same experimental conditions in subjects meeting the inclusion and exclusion criteria.
Design
An IRB approved 6 week study that included a 3 week randomized, sham treatment controlled, double-blind clinical trial arm followed by a 3 week open label crossover arm in which subjects in the sham and control groups could elect to participate in a treatment course of CES.
Primary Effectiveness Endpoint
알파 스팀(Alpha-Stim)®
장치
The primary effectiveness endpoint in the RCT was the change from baseline in the last post-treatment self-rated scores on the 10 point Numerical Rating Scale (NRS) for overall pain, quality of sleep, feelings of well-being and quality of life, and Profile of Mood States (POMS) subscales compared to the sham treatment group at the end of week 3 of the study.
The primary effectiveness endpoint in the open label crossover arm was the change from baseline in the last post-treatment scores on the 10 point Numerical Rating Scale (NRS) to post-test for overall pain, quality of sleep feelings of well-being and quality of life, and POMS subscales at the end of week 6 of the study. Effectiveness outcome measures were completed at the end of week 3 of the RCT study and at the end of the open label crossover arm 3 weeks later.
The primary effectiveness endpoint in the open label crossover arm was the change from baseline in the last post-treatment scores on the 10 point Numerical Rating Scale (NRS) to post-test for overall pain, quality of sleep feelings of well-being and quality of life, and POMS subscales at the end of week 6 of the study. Effectiveness outcome measures were completed at the end of week 3 of the RCT study and at the end of the open label crossover arm 3 weeks later.
Key Inclusion Criteria
• Male and female subjects with fibromyalgia ≥ 21 years of age.
• Diagnosis of fibromyalgia was verified by a board certified rheumatologist using the criteria established by the American College of Rheumatology.
• Diagnosis of fibromyalgia was verified by a board certified rheumatologist using the criteria established by the American College of Rheumatology.
Key Exclusion Criteria
• Pregnancy.
• Presence of implanted pacemakers, pumps or stimulators.
• Presence of implanted pacemakers, pumps or stimulators.
Protocol Summary Randomization assignment was established prior to the start of the study. The measurements of primary effectiveness endpoint were taken at baseline, prior to start of treatment period. No change was made in the medical management of the patient during the study. The protocol consisted of two arms:
• RCT arm: 3 weeks of treatment with either the active CES device or the sham device. Following the baseline tests, subjects were taught to use the CES device, and were instructed to use it every day for one hour over the 3 week period. At the end of 3 weeks, the subjects returned to the clinic, and outcome measures were repeated.
• Open label crossover arm: At this time blinding was broken and subjects in the sham and control groups were given the option to receive active CES for 3 weeks. 23 of the 40 subjects in the sham group elected to participate in the open label crossover arm. Subjects used the CES device daily for 1 hour for 3 weeks. At the completion of the 3 week open label crossover arm, subjects were retested on study outcome measures.
• Open label crossover arm: At this time blinding was broken and subjects in the sham and control groups were given the option to receive active CES for 3 weeks. 23 of the 40 subjects in the sham group elected to participate in the open label crossover arm. Subjects used the CES device daily for 1 hour for 3 weeks. At the completion of the 3 week open label crossover arm, subjects were retested on study outcome measures.
Device Application Protocol
Subjects were randomly assigned into 3 separate groups, ether active CES at a subsenate level, sham group or control by drawing subjects names out of a container. The active CES device was set to 100 µA, a subsensory level. The sham device was identical in appearance to the active CES unit, but used ear clips made for this study that did not conduct an electrical current.
Study Blinding
The subjects, investigators, physicians and staff were all masked as to the identity of the device.
Outcome Measures
The Profile of Moods (POMS) subscale A was used to measure anxiety and the POMS subscale D was used to measure depression. Sleep quality was measures by a 10 point numerical rating scale. All scales used have established reliability and validity (McNair et al., 2014, 1971; Farrar et al., 2008).
Results
Subjects
A total of 60 subjects were enrolled, 58 females and 2 men ranging in age from 23 – 82 (M = 50) years of age. All 60 subjects completed the post-testing at the completion of the last treatment at the end of their week 3 visit. The average duration of symptoms was 11 years (range 1 – 40 years). Subjects were randomized to the active CES group (N=20), sham group (N=20) or a wait-in-line placebo control group (N=20).
Baseline Measurements: Group Equivalence
There was no statistically significant difference at baseline between active CES and sham treatment groups on any of the 12 outcome measures.
Data Analysis
In December 2011, the data from this 2001 Lichtbroun study were reanalyzed to by Dr. Larry Price, statistical consultant to Electromedical Products International, Inc. to verify the findings previously reported and to conduct additional more powerful analyses that could provide a more comprehensive description of the findings. The raw data was analyzed using analysis of covariance (ANCOVA) and Mann-Whitney U. The investigators originally used a one-way analysis of variance (ANOVA) to comparing baseline and endpoint study outcomes
Primary Effectiveness Results: Week 3
The active CES group had significant findings on 8 of the 11 variables compared to the sham group: significantly lower anxiety scores (p=0.04, d = -.60), higher quality of sleep scores (p = 0.02,d = .45), lower pain scores (p = .004, d = .65), higher feelings of well-being scores (p = .007, d = .73), higher quality of life scores (p =.000, d = .97), lower fatigue scores (p = 0.03, d = -.72 and lower anger scores (p = 0.04, d = .60) compared to sham group (See Table 1). The treatment effect sizes between active CES and sham group ranged from -.36 to .97 on 8 significant variables, with a pooled effect size of .64. Table 1shows results of statistical analyses of outcome measures and Figures 1 and 2 show the results between groups in anxiety scores and sleep quality.
|
|
|
Open Label Crossover Results: Week 6
After completion of the RCT arm, 23 of the 40 sham or control patients opted for actual CES in an open label crossover arm where they could increase the current in accordance with the standard clinical protocols for Alpha-Stim CES. Data were analyzed with repeated measures analysis of covariance variance, with least significant difference a posteriori testing. Table 7 shows results of statistical analyses of outcome measures at week 6.
|
Quality of the Research
Strengths of this study are: use of a randomized, sham controlled, double-blind design (the investigators chose to use the Alpha-Stim RCT research protocol for the study); active and sham Alpha-Stim devices were pre-set and locked at the designated levels for each specific group for current level and time by the manufacturer at the factory and sham units were the same as active units, except they did not emit electricity; randomization of devices was done by the manufacturer and followed according to the protocol by the investigators; use of 3 groups, active sham and the control group; and the structured and detailed protocol for the CES treatments for both active and sham groups. A limitation of the original data analysis is that it used analysis of variance (ANOVA) and no within or between group effect sizes were included. In the 2011 reanalysis of the data, analysis of covariance (ANCOVA) was used to provide a more comprehensive description of the findings. The Profile of Mood States (POMS) subscales were used to measure anxiety and depression. This was a common approach in the late 1990s and early 2000s. Today, the Hamilton Anxiety Rating Scale or similar rating scale that focuses entirely on the anxiety would most likely be used. The same is true for measuring the variable of depression. The effect of CES on depression was not significant in this study in contrast to the findings of other Alpha-Stim studies on depression. One possible explanation for this finding is the use of the POMS subscale on depression, whereas other studies used scales that focused specifically on depression, such as the Hamilton Depression Rating Scale. The findings for anxiety and sleep quality in this study are consistent with the findings of other Alpha-Stim studies that found CES significantly decreases anxiety and improves sleep quality.
Author Affiliations
ASL, Robert wood Johnson Medical School, East Brunswick, NJ. MMC, Real Word Health, Wall, NJ. RBS, Electromedical Products International, Mineral Wells, TX,
References
Farrar JT, Troxel AB, Stott C, Duncombe P, Jensen MP. Validity, reliability, and clinical importance of change in a 0-10 numeric rating scale measure of spasticity: a post hoc analysis of a randomized, double-blind, placebo-controlled trial. Clinical Therapeutics. 2008 May;30(5):974-85
McNair DM, Lorr M, Droppleman LF. Profile of Mood States 2nd Editon (POMS 2™). JvR Psychometrics, Accessed on 4/18/2014, http://www.psychologyafrica.com/wp-content/uploads/2013/07/Profile_of_Mood_States_2nd_Edition.pdf,
McNair DM, Lorr M, Droppleman LF. Manual for the Profile of Mood States. San Diego, CA: Educational and Industrial Testing Service, 1971.
출처: 알파스팀제조사 EPI 홈페이지
| 목록으로 가기 |




